What is an Orthodontist?
An orthodontist is a dentist who has completed at least 3 years of extra training to specialize in orthodontics. An orthodontist can register with the National Specialist Register of Malaysia.

I am interested in braces. Can you tell me more?
If you choose to have braces done, required diagnostic information (eg. dental impressions, photographs and X-rays) will be obtained on your first visit.
Once all diagnostic information has been obtained, we will discuss all aspects of your orthodontic treatment with you at the subsequent visit.
How much do braces cost?
The fee for braces depends on many factors (eg. type of braces, additional accessories).
For more information, click here
What are the benefits of having braces done?
- Improve your smile.
- Facilitate maintenance of oral hygiene.
- Retract/pull back protruding front teeth.
- Reduce damage to the gums from improper bite.
- Straighten teeth which have undergone “drifting” in patients with gum disease (periodontitis).
- Facilitate placement of denture, bridge or implant.
- Improve self-esteem and confidence.
I do not like the look of metal braces. What are my options?
- Clear braces (eg. ceramic, composite)– these clear brackets are more aesthetically pleasing. They cost more and are more brittle. These brackets are very popular amongst adults as well as some teens.
- Lingual braces – the brackets are fitted to the back of the teeth. Therefore, they are not visible when smiling. The drawbacks are higher cost and longer chairside adjustment time. Patients might take a longer time to adjust to the braces due to tongue irritation.
- Clear aligners – these are clear flexible plastic splints which the patient can put on and remove themselves. The most famous brand is Invisalign but there are other alternative brands as well. They are most suitable for mild to moderate cases. The disadvantages are high cost and high patient compliance as they must be worn for at least 22 hours a day.




What are the different parts of braces? What are the colourful things on the braces?

- Brackets are attachments which are glued to the teeth. Brackets can be made of stainless steel, titanium, plastic, ceramic or composite.
- Archwires are placed on the brackets to move teeth. Archwires can be made of stainless steel, nickel-titanium alloy or titanium-molybdenum alloy (TMA/beta titanium).
- The archwires are secured to the brackets using coloured elastic modules.
- Some brackets (ie. Self-ligating brackets) have special clips which hold the archwires in place without the need for elastic modules.
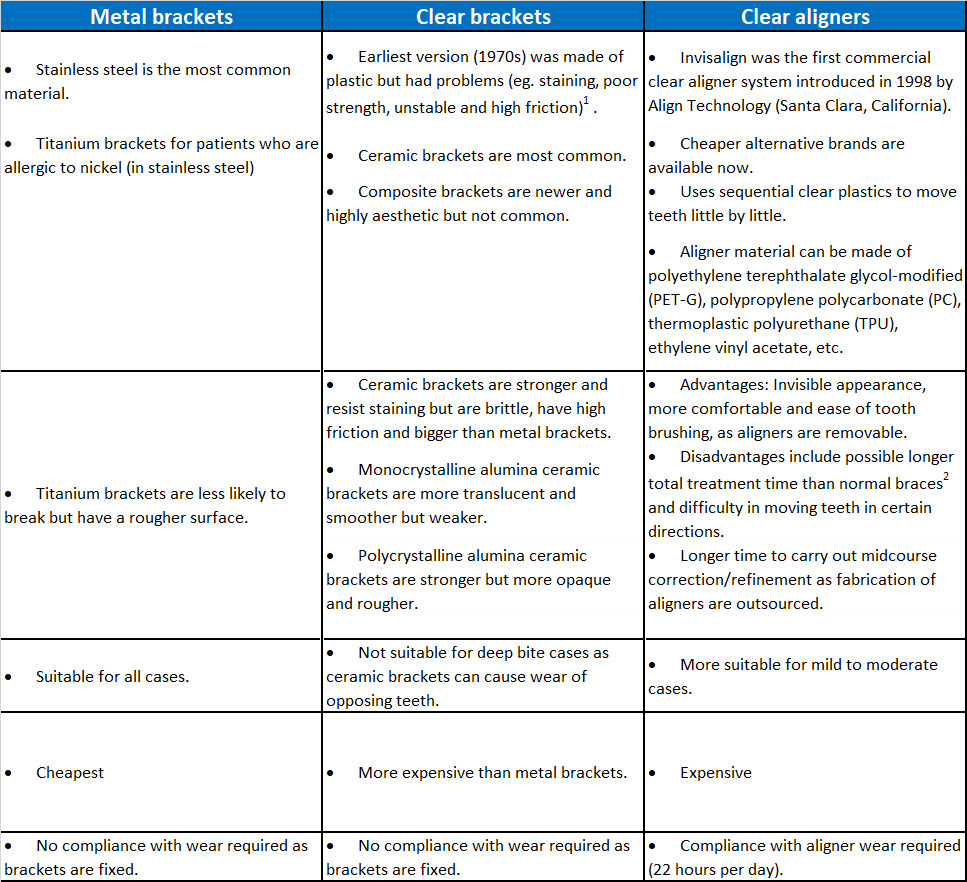
Comparison between metal braces, clear braces and clear aligners (eg. Invisalign)
- Prior to the 1970s, brackets were welded to metal bands/rings. The bands were then fitted around the teeth (see below). The fitting process was arduous, time-consuming and uncomfortable.

Full Mouth Banding (Source: Begg PR, Kesling PC. Begg Orthodontic Theory and Technique. 3rd ed. Philadelphia: WB Saunders; 1977)
- Around the 1970s, dental cements were developed which allowed direct bonding of brackets to teeth.
- Metal brackets are produced using 3 methods:
- Metal-injection moulding (MIM) – most common
- Casting
- Computer-aided design and computer-aided manufacturing (CAD-CAM).
- With the CAD-CAM method, there are 2 principle techniques: milling and rapid prototyping (3-D printing).
- CAD-CAM method can be used to manufacture metal or clear brackets and they are smoother and more precise.
What are Damon braces?

- Damon braces are self-ligating brackets. This means that the brackets have clips to hold the archwires in place and elastic modules are not required. There are many different brands of self-ligating brackets but Damon is probably the most well-known brand currently.
- Damon brackets, and self-ligating brackets in general, have been inaccurately presented as a separate and more superior type of braces.
- In reality, self-ligating brackets are sub-types of metal or clear brackets.
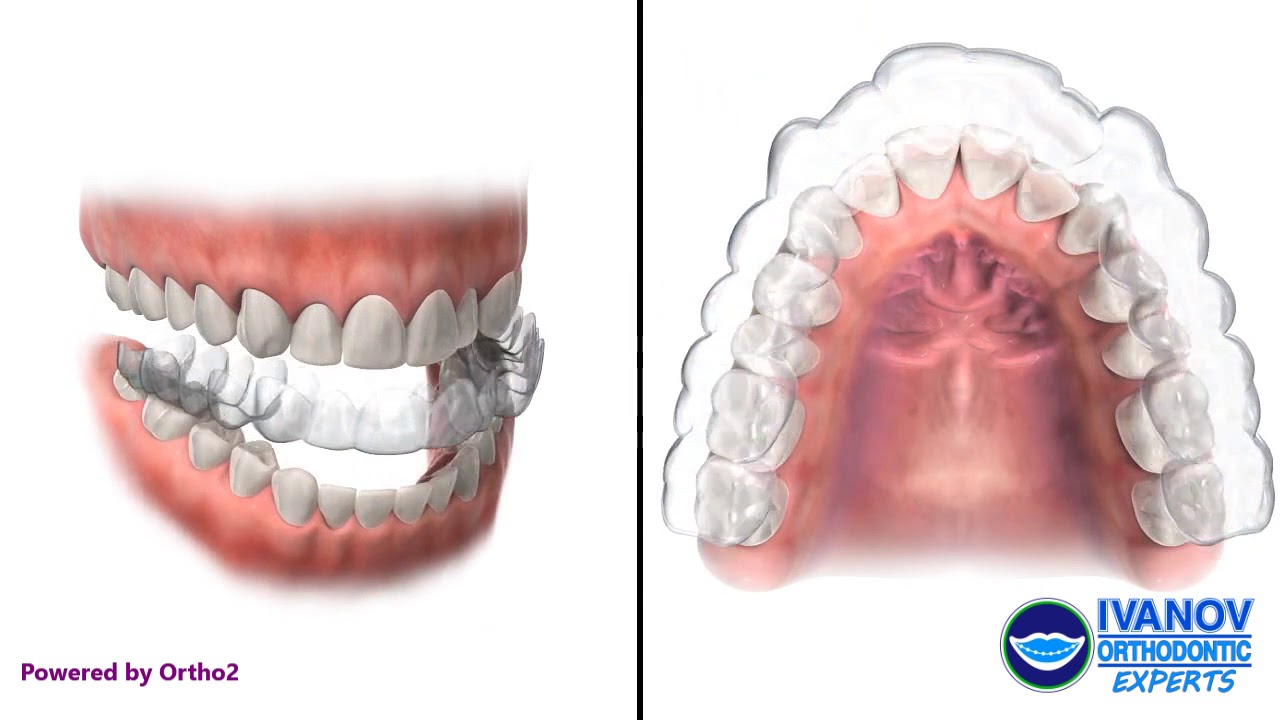
How do clear aligners (eg. Invisalign) work?

Do I need to have extractions for braces?
It depends. Usually extractions of teeth are required to provide space to straighten crooked teeth. Sometimes teeth are extracted so that the protruding front teeth can be pulled back.
Do braces hurt?
The process of fitting the braces do not hurt. Some discomfort during eating is expected following fitting of the braces. The pain and discomfort normally last for a few days up until a week. Painkillers (eg. Paracetamol) can be taken if the pain is unbearable.
How often do I need to come for appointments?
Appointments are normally scheduled every 4-6 weeks.
How long does treatment with braces take?
Treatment duration varies between patients and can take about 2 years to complete. More complex cases can take even longer.
What are the common problems associated with braces?
- Brackets can come off if you bite on something hard. It is advisable to avoid hard and chewy food throughout the duration of treatment.
- Pain or discomfort. There may be some discomfort in the first few days but the discomfort should go off after a week.
- Poor oral health. Cavities, white spot lesions (demineralization of the enamel) and gum disease can happen if excellent oral hygiene is not maintained.
- Multiple appointments. Braces treatment can take up to 2 years or more to complete. If you are planning to move abroad (eg. for studies) within that time, then it may be advisable to defer treatment.
What happens after the braces come off?
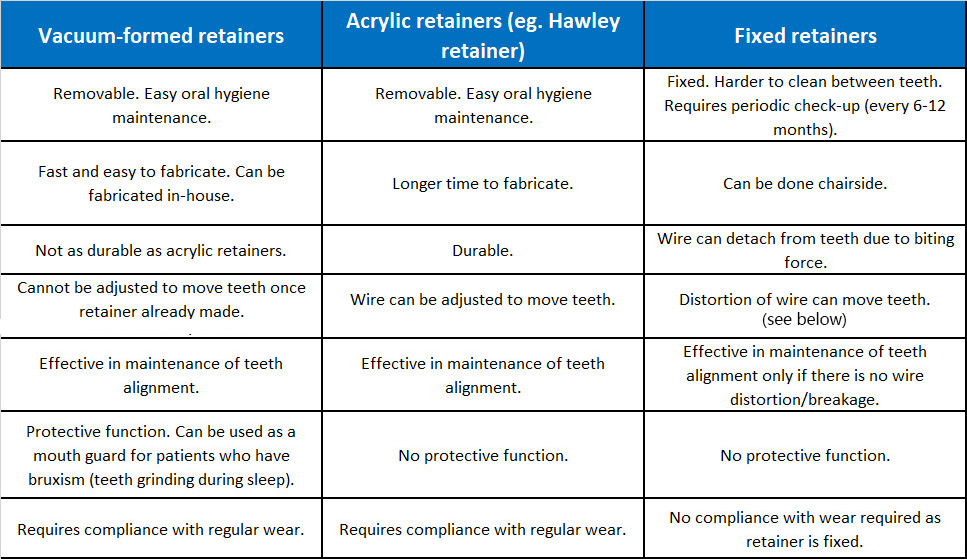
- Vacuum-formed retainers – these are clear plastic splints which can double as mouth guards if patients grind their teeth during sleep
- Acrylic retainers (eg. Hawley retainers) – these are made of acrylic/plastic and metal wires

- Fixed retainer – these are wires glued to the back of teeth. Periodic check-ups are necessary in case the wire detaches from the teeth.
Oral hygiene must be excellent to prevent gum problems.
Comparison between vacuum-formed, acrylic and fixed retainers

Breakage of fixed retainer causing teeth movement.
Source: Proffit WR, Fields HW, Larson B, Sarver DM. Contemporary Orthodontics. 6th ed. Missouri: Mosby; 2018.
Why do you need to wear retainers?

Reorganisation of gum (periodontal ligament) fibers around the teeth.
- After braces are removed, the gum (periodontal ligament) fibers around the teeth will reorganise to accommodate the new tooth positions.
- The process happens over a 3-4 month period.
- The retainers function to stabilise the tooth positions.
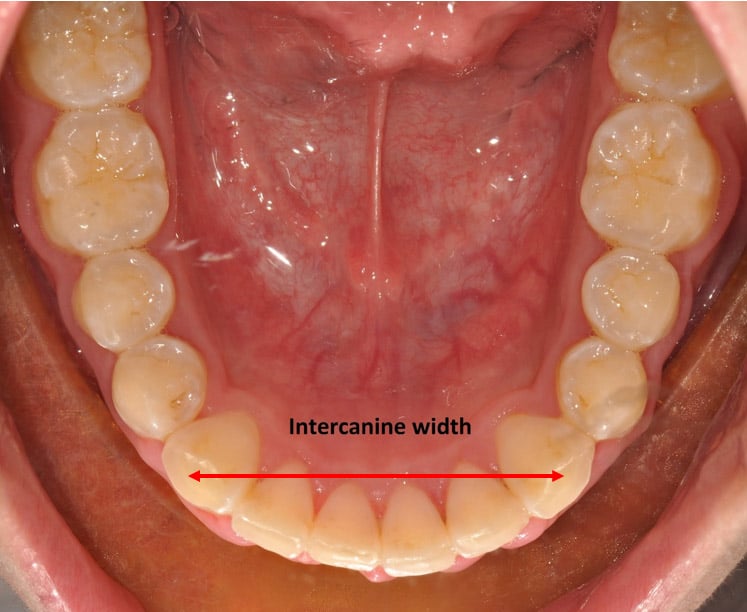
Progressive narrowing of the intercanine width (see below) with age1,2.
- The constriction of the dental arch with age will result in the lower front teeth becoming crooked again if retainers are not worn.
1. Sinclair R, Little R. Maturation of untreated normal occlusions. Am J Orthod Dentofacial Orthop. 1983;83:114-123.
2. Tsiopas N, Nilner R, Bondermark L, Bjerklin K. A 40 years follow-up of dental arch dimensions and incisor irregularity in adult. Eur J Orthod. 2013;35:230-235.
How long do I need to wear retainers for?
- The most common advice is to wear the retainers for as long as you want straight teeth.
- This would normally mean lifelong retainer wear.
- A study found that 2 out of 3 patients who stopped wearing retainers completely developed crooked lower teeth (crowding) after about 10 years1.
1. Little R, Wallen T, Reidel R. Stability and relapse of mandibular anterior alignment – first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1981;80:349-365.
Do wisdom teeth (third molars) exert pressure on the front teeth and cause the teeth to become crooked?
- It is common belief that buried (impacted) wisdom teeth (third molars) can “push” the front teeth causing them to become crooked (crowding).
- This is not entirely true as patients who do not have wisdom teeth (congenitally missing) or already had the wisdom teeth removed still developed crowding of the teeth¹.
1. Zawawi KH, Melis M. The role of mandibularl third molars on lower anterior teeth crowding and relapse after orthodontic treatment: A systematic review. ScientificWorldJournal. 2014;2014:615429.
When should I remove my wisdom teeth (third molars)?
You should consider having your wisdom tooth/teeth removed in the following conditions¹:



- Recurrent pericoronitis. Repeated episodes of gum swelling around the wisdom tooth.
- Decay (caries) of the wisdom tooth. If it is difficult to clean the area surrounding the wisdom tooth, it might be preferable to extract the wisdom tooth. (Figure 1)
- Decay (caries) of adjacent tooth. If the adjacent tooth is decayed, then removal of the wisdom tooth is necessary to allow filling to be done. (Figure 1)
- Infection. Pericoronitis or decayed wisdom tooth can cause infection of the area around the wisdom tooth.
- Periodontitis. Gum disease (periodontitis) can occur around wisdom tooth. A study showed that 1 in 4 person with non-problematic wisdom teeth had gum disease around the wisdom teeth area².
- Nonfunctional wisdom tooth. If the opposing wisdom tooth is missing (either extracted or congenitally missing), then the wisdom tooth may need to be removed. This is to prevent trauma of the gums on the opposing side due to elongation of the tooth (supraeruption). Figure 2.
- Denture covering buried (impacted) wisdom tooth. If the buried wisdom tooth is very near the gums, then the tooth might need to be removed to prevent irritation from the denture.
- Obstruction of adjacent tooth. If both the wisdom tooth and the adjacent tooth (second molar) are buried, then the wisdom tooth might need to be removed to allow the second molar to be straightened. (Figure 3)
- Jaw surgery with braces. If jaw surgery is planned for the lower jaw, then the lower wisdom teeth would need to be removed at least 6 months before surgery to facilitate the jaw surgery procedure.
1.Steed MB. The indications for third-molar extractions. J Am Dent Assoc. 2014;145(6):570-573.
2. Blakey GH, Marciani RD, Haug RH, et al. Periodontal pathology associated with asymptomatic third molars. J Oral Maxillofac Surg 2002;60(11):1227-1233.
When should a child first see an orthodontist?
Early orthodontic treatment can be carried out in children between the ages of 7 to 12. Most children start having braces around the age of 12 or when all their permanent teeth (except wisdom teeth) have come through.
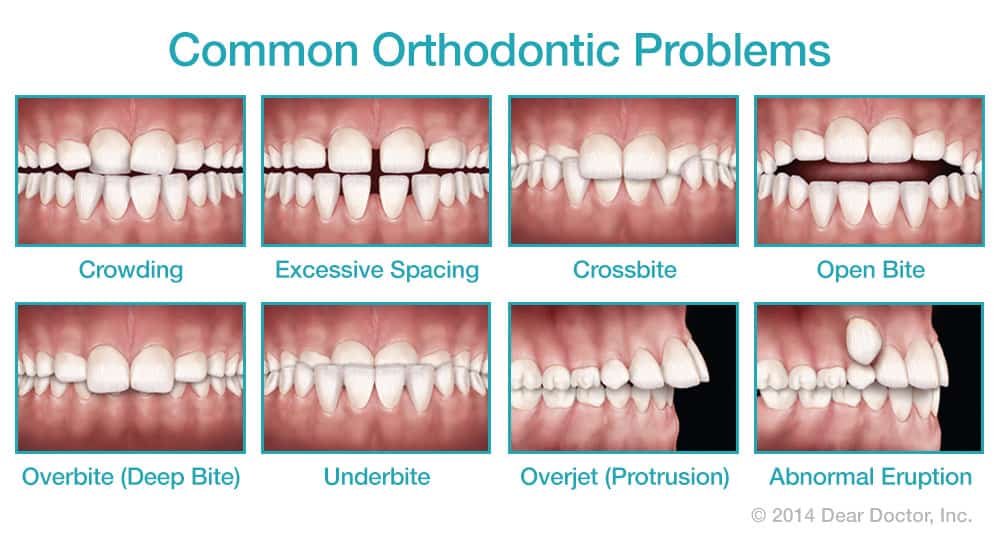
What kind of common problems can be treated early?
- Deep bite - when the upper front teeth overlap the lower front teeth too much.
- Cross bite – when the upper teeth bite behind/inside the lower teeth
- Open bite due to oral habits (eg. finger sucking) – when the upper and lower front teeth do not meet
- Over-retained milk teeth – when the milk teeth have not fallen out even when the replacement permanent teeth are almost fully formed
- Supernumerary teeth – extra teeth in the mouth
- Deficient lower jaw – when the lower jaw is positioned further back compared to the upper jaw
How can the problems be treated early?
- Removable appliances – acrylic/plastic plates with wires designed to move teeth

- Functional appliances – acrylic/plastic plates designed to modify jaw growth

- Partial fixed appliance – fixed braces only on a few teeth (2x4 appliance)

Will I still need braces after early orthodontic treatment?
It depends. Some problems can be resolved without further treatment at a later stage. In some other cases, early treatment only reduces the severity of the problem and the child would need comprehensive treatment with braces later.